
If you buy something using links in our stories, we may earn a commission. Learn more.
At this point it’s been made to seem like common sense: Larger-bodied people are at higher risk from this pandemic. “Those who are overweight really need to be careful,” France’s chief epidemiologist declared last week. “That is why we're worried about our friends in America.”
In recent weeks, many news outlets—and a few scientific journals—have sent the same frightening message. A study posted on a preprint server last weekend by researchers at New York University provided fodder for the latest round of this reporting: “Obesity appears to be one of the biggest risk factors related to Covid-19 hospitalizations and critical illness,” Newsweek claimed on Tuesday. Yet this rhetoric is based on flawed and limited evidence, which only exacerbates the stigma that larger-bodied people already face in society and our health care system. That stigma is what truly jeopardizes their health, not weight itself—a fact that’s only more important to consider in the midst of this pandemic.
To date, the most plausible research pointing to higher BMI as a risk factor includes three preliminary reports that have been released since April 8: a Centers for Disease Control and Prevention report with descriptive statistics on people who’ve been hospitalized for Covid-19, showing that 48 percent of those with available BMI data are in the “obese” category (a slightly higher percentage than the 42 percent in the US as a whole); a small French study that found people with a BMI of 35 and above are at higher risk of being put on a ventilator; and a letter to the editor of the journal Clinical Infectious Diseases from researchers at NYU’s School of Medicine (including one of the authors of last week’s preprint), sharing a preliminary finding that people with a BMI of 30 or above appear to be at higher risk for hospitalization and intensive-care admission, if they’re less than 60 years old. (Among people who are 60 or older, weight status did not seem to be important.)
All of these reports are flawed in similar ways. Most important, none of them control for race, socioeconomic status, or quality of care—social determinants of health that we know explain the lion’s share of health disparities between groups of people. Structural racism and other forms of inequality in our society have long been linked to worse health outcomes, including higher rates of diabetes and hypertension (two likely Covid-19 risk factors) among people in oppressed groups. Now, those health disparities are on full display in the Covid-19 pandemic, which is disproportionately impacting black communities—not because of biology, but because of systemic inequalities like higher rates of exposure to the virus and less access to medical care.
As it happens, that recent preprint from NYU did take race into account, in its finding that having a very high BMI was a major risk factor for hospitalization. But the same analysis also found that BMI was only marginally important at predicting which hospitalized patients would go on to have “critical” illness. It also seemed to indicate that being African American was in some way significantly protective against Covid-19: Black patients admitted to the hospital were only half as likely as white patients to develop the most serious symptoms, according to the study. Needless to say, few if any outlets touted this dubious result.
Another glaring issue with the three published reports about BMI and Covid-19: They don’t control for known individual health risks that may be associated with worse outcomes for this virus, including asthma and other chronic respiratory conditions, cancer, and immunosuppressive medication use. The CDC report and NYU letter to the editor don’t control for diabetes or cardiovascular conditions, either, although these two likely risk factors for Covid-19 happen to be associated with higher BMI. The French study of 124 patients does control for diabetes and hypertension, as well as dyslipidemia, but not for other risk factors—even though in the study’s introduction, the authors themselves acknowledge that cardiovascular disease, chronic respiratory disease, and cancer are also likely to raise the risk of Covid-19.
Moreover, these reports all fail to control for the particular ways in which clinicians’ biases and beliefs about body size are likely to be influencing Covid-19 care decisions for higher-weight people. In 2013, the American Medical Association labeled “obesity” as a disease (against the recommendation of the AMA’s internal committee devoted to studying the matter), and the CDC has included a BMI of 40 or above on its list of risk factors for severe Covid-19 illness since mid-March. So higher-weight people may be more likely to get hospitalized simply because they’re viewed as unhealthy and deemed higher-risk patients. The April 8 CDC report only includes BMI measurements for 10 percent of the patients in the sample, and while it’s understandable that they’d have so much missing data amid the chaos of a global pandemic, it’s also possible that higher-weight people are more likely to be weighed because their weight is assumed to be clinically relevant. Thus, people with a high BMI could just be overrepresented in the data.
Where did the CDC get the idea that people with a BMI of 40 or above are at greater risk in the first place? It’s unclear. A CDC press contact didn’t respond to a request for comment, but the peer-reviewed evidence that was available at the time the agency made that pronouncement generally indicated weight was not a risk factor. Nearly all published data from China (where Covid-19 has been studied since first being discovered in December 2019) shows that high BMI alone isn’t associated with developing the disease or with having a critical outcome. In most Chinese studies, high BMI doesn’t even make the list of preexisting conditions among Covid-19 patients—despite the fact that one-third of China’s population has a BMI in the “overweight” or “obese" categories, and that China considers weight management a public-health priority. Early US reports from public health departments also seemed to indicate that higher BMI isn’t a risk factor: In New York State, for example, “obesity” hasn’t been on the state’s list of the top 10 preexisting conditions associated with Covid-19 fatality as of this writing. The “obesity” rate documented among some of the earliest Covid-19 cases in Washington’s King County matched that of the county as a whole.
What’s more, the (limited) data available on deaths and BMI so far suggest we could end up seeing a lower risk of death among higher-weight people. For example, the Louisiana health department is reporting as of April 16 that 22 percent of the people who’ve died of Covid-19 in Louisiana were in the “obese” BMI category, but nearly 37 percent of the state’s overall population falls into that category, according to the CDC.
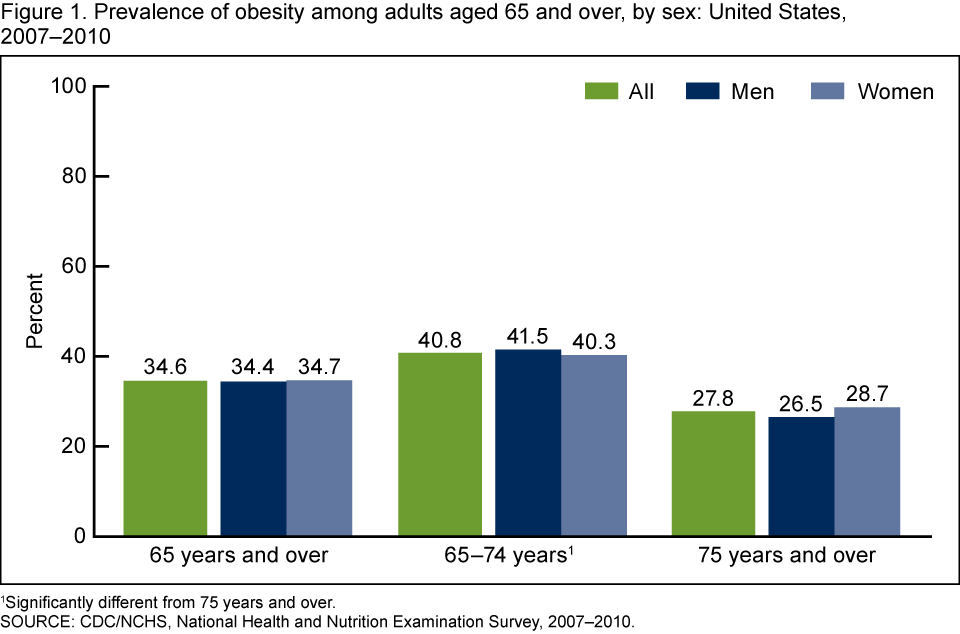
Some of that could be an artifact of differences in age or sex. Age is clearly the biggest factor affecting the case fatality rate of Covid-19, and in general elderly adults tend to be smaller-bodied because of age-related losses in both fat and muscle mass. Another confounding factor could be that women are more likely to have BMIs in the “obese” category than men, and yet female sex seems to be a protective factor against Covid-19.
Still, the early numbers suggest it’s possible that being in that BMI category could actually be protective against Covid-19 death. That might sound outrageous, given the conventional wisdom that “obesity kills,” but there’s evidence to indicate that heavier people may have some protection against at least one of the major sources of Covid-19 mortality: acute respiratory distress syndrome (ARDS). A 2017 meta-analysis found that having a BMI of 30 or above was associated with a significantly lower risk of dying from ARDS, compared to those in the “normal” category. And ARDS isn’t the only condition where we see this pattern; higher BMI is associated with a lower risk of adverse outcomes in many diseases and clinical situations, such as pneumonia survival, sepsis, heart failure, and diabetes hospitalization and survival—the so-called “obesity paradox.”
Yet all of that early evidence didn’t stop researchers and editors of medical journals from speculating that high BMI was going to emerge as a risk factor. These groups were extrapolating from the evidence on H1N1 influenza (aka swine flu), where some data suggested this was true. But a 2016 meta-analysis of studies on H1N1 and weight points to different conclusions: For one, there’s no increased risk of death from swine flu for people with BMIs of 25 and above. And though it first appeared that people in this group did have an increased risk of having severe, nonfatal complications, those associations disappeared after the researchers adjusted for an important confounding variable: Smaller-bodied H1N1 patients were more likely to get early antiviral treatment. It turned out that lower-quality health care, not high BMI, was responsible for the increased risk seen in people with BMIs in the “obese” category.
That’s weight stigma, and it’s the real issue here. Anti-fat bias has been linked to sub-par health care in a variety of ways, including providers spending less time with larger-bodied patients; speaking more curtly and less compassionately to them; and misattributing symptoms to their weight instead of referring them for testing or offering evidence-based, non-weight-related treatment options. Discrimination against higher-weight people is a known, independent risk factor for all kinds of health problems that typically get blamed on weight, including diabetes and heart disease. And Covid-19 is only amplifying this preexisting disparity. “When you take that and then you throw a pandemic on top, it’s like adding water to a grease fire,” says Joy Cox, a researcher at Rutgers New Jersey Medical School. “Health disparities that weren’t addressed when there was an opportunity to address them have been magnified.”
The fact that researchers have been pointing to body size as a risk factor for weeks now, even in the absence of much evidence, is a clear example of how weight stigma gets enacted in science. “Consider the questions of whether high-BMI folks are at increased risk for contracting Covid-19—and if they do contract it, whether they have poorer outcomes,” says Lindo Bacon, a weight-science researcher and author of the books Health at Every Size and Body Respect. “First, notice the bias built into the questions. There is some indication that opposing hypotheses are better supported by current research—whether they are at lower risk, and have better outcomes—but I haven’t seen anyone frame their questions that way yet.”
Indeed, multiple studies have found that simply reading a news article about the so-called “obesity epidemic” induces weight stigma and increases the expression of anti-fat attitudes among participants. Reports about the pandemic that name body size as a risk factor likely do the same. “I suspect that this news coverage constantly linking weight to Covid-19 risk is also heightening anti-fat bias,” says Jeffrey Hunger, a researcher who studies the effects of weight stigma and other forms of discrimination at Miami University of Ohio. “This constant barrage of media coverage linking weight to Covid-19 might lead to blaming individuals for actually contracting it.” And from my interactions with dozens of higher-weight clients, readers, and podcast listeners, it’s clear that many people are feeling blamed and shamed right now. “In a lot of ways it does make you feel like it’s your fault,” says Cox, who is at a higher weight. That feeling of self-blame just worsens the already difficult situation of living through a global pandemic. “There's an extra mental and emotional toll that it takes,” Cox says.
Instead of trumpeting the supposed risks of high BMI and adding to the already damaging impact of weight stigma, researchers need to be asking deeper questions, and public health officials and journalists need to report on the science in more nuanced and sensitive ways. To do otherwise is to create the very outcomes that we want to avoid.
Photographs: Nathan Laine/Bloomberg/Getty Images; Ludovic Marin/AFP/Getty Images
WIRED Opinion publishes articles by outside contributors representing a wide range of viewpoints. Read more opinions here. Submit an op-ed at opinion@wired.com.
- Why are some people getting so sick? Ask their DNA
- “Here in spirit”: an oral history of faith amid the pandemic
- Un-miracle drugs could help tame the pandemic
- WIRED Q&A: We are in the midst of the outbreak. Now what?
- What to do if you (or a loved one) might have Covid-19
- Read all of our coronavirus coverage here











{kind=link}